NCLEX pharmacology is not about memorizing every medication in the drug book.
That is not realistic.
The exam usually tests whether you can recognize medication patterns, connect drugs to labs and vital signs, and choose the safest nursing action.
You need to know common drug classes.
You also need to know what can harm the client fastest.
That means:
- Side effects
- Contraindications
- Toxicity signs
- Antidotes
- Therapeutic levels
- Lab monitoring
- Vital sign parameters
- Patient teaching
- High-alert medication safety
What NCLEX pharmacology questions test
NCLEX pharmacology questions may ask you to:
- Identify an adverse effect
- Hold a medication based on a vital sign
- Question a prescription
- Recognize a toxic drug level
- Select patient teaching
- Match a medication to a lab value
- Prioritize which client to assess first
- Choose an antidote
- Identify a contraindication
- Notice a drug interaction
- Prevent a medication error
- Evaluate whether the medication worked
Pharmacology can appear in regular multiple-choice questions and in Next Gen NCLEX case studies.
You may see a medication administration record, labs, vital signs, provider orders, and nurses’ notes all in the same item.
For a full medication-pattern review, use NurseZee’s pharmacology flashcards for 50 high-yield drug classes with this guide.
Why pharmacology feels hard
Pharmacology feels hard because it combines several subjects at once.
A question about furosemide is not only about furosemide.
It may also test:
Potassium
Blood pressure
Dehydration
Fall risk
Kidney function
Ototoxicity
Heart failure symptoms
Daily weights
Intake and outputThat is why memorizing one-line definitions is not enough.
You need to understand how medications affect real clients.
The NCLEX medication name rule
The NCLEX uses generic medication names on most items.
Study:
acetaminophen
furosemide
lisinopril
metoprolol
warfarin
heparin
insulin lispro
sertralineDo not build your study plan around brand names.
Brand names can help in clinical practice, but generic names are the safer NCLEX focus.
The 7 golden rules of NCLEX pharmacology
Rule 1: Know the class before the single drug
You do not need to memorize every medication individually.
You need class patterns.
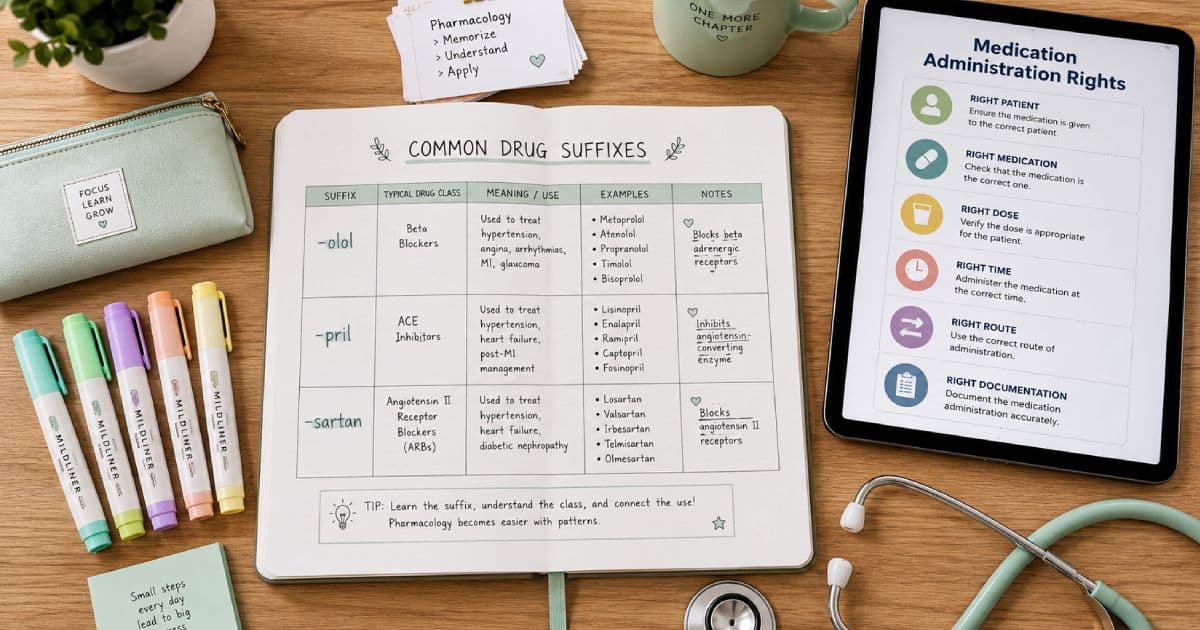
If you recognize that a drug ending in -pril is an ACE inhibitor, you can predict:
- Low blood pressure
- Hyperkalemia
- Dry cough
- Angioedema
- Pregnancy risk
- Need to monitor kidney function and potassium
Rule 2: Connect every medication to one safety check
Ask:
What do I check before giving this?| Medication | Check before giving |
|---|---|
| Digoxin | Apical pulse, potassium, toxicity signs |
| Beta-blocker | Heart rate, blood pressure, asthma/COPD caution |
| ACE inhibitor | Blood pressure, potassium, renal function, pregnancy status |
| Furosemide | Potassium, blood pressure, dehydration, kidney function |
| Heparin | aPTT or anti-Xa per protocol, platelets, bleeding |
| Warfarin | INR, bleeding, pregnancy status, diet consistency |
| Insulin | Blood glucose, meal status, insulin type |
| Opioid | Respiratory rate, sedation level, blood pressure |
| Lithium | Lithium level, sodium/fluid status, kidney function |
| Theophylline | Drug level, heart rate, toxicity signs |
Rule 3: Side effect is not always emergency
A side effect can be expected.
An adverse effect can be dangerous.
A life-threatening reaction is priority.
Lower-priority expected effects
Usually not first priority if mild:
- Mild nausea
- Dry mouth
- Mild headache
- Mild dizziness after first dose
- Constipation from opioids
- Dark stools with iron
- Orange urine with rifampin
- Metallic taste with metronidazole
Higher-priority red flags
Usually urgent:
- Angioedema
- Stridor
- Wheezing after medication
- Respiratory depression
- Severe hypotension
- Chest pain
- New confusion
- Severe bleeding
- Black/tarry stool with anticoagulants
- Platelet drop on heparin
- Potassium 6.2 mEq/L
- Severe hypoglycemia
- Stevens-Johnson syndrome signs
- Serotonin syndrome signs
- Neuroleptic malignant syndrome signs
Rule 4: Labs are medication safety clues
NCLEX will often give a medication administration record, labs, and vital signs.
Do not skip the labs.
| Lab | Medication concern |
|---|---|
| Potassium | Digoxin, ACE inhibitors, ARBs, spironolactone, loop diuretics |
| INR | Warfarin |
| aPTT or anti-Xa | Heparin protocols |
| Platelets | Heparin, enoxaparin, chemotherapy, antiplatelets |
| Creatinine/eGFR | Vancomycin, aminoglycosides, metformin, digoxin, lithium |
| Liver enzymes | Acetaminophen, statins, isoniazid, valproate |
| Glucose | Insulin, corticosteroids, diabetes medications |
| Lithium level | Lithium |
| Digoxin level | Digoxin |
| Phenytoin level | Phenytoin |
| Theophylline level | Theophylline |
Rule 5: High-alert medications need double-check thinking
High-alert medications can cause major harm if used incorrectly.
NCLEX loves these because they test safety.
Examples include:
- Insulin
- Heparin
- Warfarin
- Enoxaparin
- Opioids
- Sedatives
- Neuromuscular blockers
- Concentrated electrolytes
- Chemotherapy
- Vasopressors
- IV potassium
- Magnesium sulfate
- Parenteral nutrition
When you see a high-alert drug, slow down.
Ask:
Is this the right patient, right drug, right dose, right route, right time, right indication, and right monitoring?Rule 6: Never ignore allergy, pregnancy, or organ function
Common NCLEX contraindication clues:
| Clue | Medication concern |
|---|---|
| Pregnancy | ACE inhibitors, ARBs, warfarin, isotretinoin, many anticonvulsants |
| Asthma/COPD | Nonselective beta-blockers |
| Kidney disease | Aminoglycosides, lithium, metformin, digoxin dose concerns |
| Liver disease | Acetaminophen, statins, valproate, isoniazid |
| Active bleeding | Anticoagulants, antiplatelets, NSAIDs |
| Peptic ulcer disease | NSAIDs, corticosteroids with caution |
| Bradycardia | Beta-blockers, digoxin, some calcium channel blockers |
Rule 7: Patient teaching must match the safety risk
Good teaching is specific.
Weak teaching:
Take this medication as prescribed.Better teaching:
Take warfarin at the same time each day. Keep vitamin K intake consistent. Report black stools, blood in urine, severe headache, unusual bruising, or bleeding that does not stop.NCLEX drug suffixes and name clues
Suffixes are shortcuts.
They are not perfect.
Use them to recognize a class, then confirm with the question context.
| Suffix or clue | Common class | NCLEX safety focus |
|---|---|---|
-pril | ACE inhibitors | Cough, hyperkalemia, angioedema, pregnancy risk |
-sartan | ARBs | Hyperkalemia, pregnancy risk |
-olol | Beta-blockers | Bradycardia, hypotension, bronchospasm caution |
-dipine | Calcium channel blockers | Hypotension, edema, headache |
-statin | HMG-CoA reductase inhibitors | Myopathy, liver enzymes, grapefruit caution for some drugs |
-semide | Loop diuretics | Hypokalemia, dehydration, ototoxicity |
-thiazide | Thiazide diuretics | Hypokalemia, hyperglycemia, photosensitivity |
-prazole | Proton pump inhibitors | Long-term fracture/C. diff/magnesium concerns |
-tidine | H2 blockers | Confusion risk in older adults, renal dosing |
-cillin | Penicillins | Allergy, anaphylaxis |
cef- or ceph- | Cephalosporins | Allergy, diarrhea, infection treatment |
-floxacin | Fluoroquinolones | Tendon injury, QT risk, CNS effects |
-cycline | Tetracyclines | Photosensitivity, teeth/bone concerns |
-azole | Antifungals | Liver concerns, interactions |
-vir | Antivirals | Kidney function, adherence |
-pam or -lam | Benzodiazepines | Sedation, falls, respiratory depression with opioids |
-oxetine, -traline, -pram | SSRIs | Serotonin syndrome, suicidality warning, bleeding risk |
-gliptin | DPP-4 inhibitors | Pancreatitis signs |
-gliflozin | SGLT2 inhibitors | UTI/genital infection, dehydration, ketoacidosis warning |
-tide | GLP-1 receptor agonists | GI effects, pancreatitis signs |
High-yield cardiovascular medications
Cardiac medications show up often because they connect to perfusion, blood pressure, electrolytes, and rhythm.
ACE inhibitors: -pril
Examples:
- lisinopril
- enalapril
- captopril
Common uses:
- Hypertension
- Heart failure
- Kidney protection in some clients with diabetes or proteinuria
- Post-myocardial infarction management
Key side effects:
- Dry cough
- Hypotension
- Hyperkalemia
- Increased creatinine
- Angioedema
Priority red flag:
Swelling of lips, tongue, face, or throat.This can signal angioedema and airway risk.
NCLEX teaching
Teach the client to:
- Rise slowly
- Report facial, lip, tongue, or throat swelling
- Avoid potassium supplements or salt substitutes unless prescribed
- Avoid pregnancy and notify the provider if pregnancy occurs
- Report persistent cough if bothersome
Example
A client taking lisinopril reports swelling of the lips and difficulty swallowing.
Priority action:
Hold the medication and assess the airway immediately.Rationale:
Lip swelling and difficulty swallowing suggest angioedema, which can progress to airway obstruction.ARBs: -sartan
Examples:
- losartan
- valsartan
- candesartan
Key side effects:
- Hypotension
- Hyperkalemia
- Renal function changes
- Pregnancy risk
Teaching:
Avoid potassium salt substitutes unless prescribed. Report dizziness, weakness, or pregnancy.Beta-blockers: -olol
Examples:
- metoprolol
- atenolol
- propranolol
- carvedilol
- labetalol
Common uses:
- Hypertension
- Angina
- Heart failure
- Rate control
- Post-MI therapy
- Some migraine prevention
Key side effects:
- Bradycardia
- Hypotension
- Fatigue
- Dizziness
- Masked hypoglycemia symptoms
- Bronchospasm risk, especially with nonselective agents
Hold parameters
A common NCLEX-style safety clue:
Heart rate less than 60/min
Systolic blood pressure low or symptomaticAlways follow the actual prescription and facility policy in practice.
On NCLEX, bradycardia or hypotension usually means the nurse should hold or question the medication.
Teaching
Teach the client to:
- Check pulse if instructed
- Rise slowly
- Do not stop suddenly
- Report wheezing or shortness of breath
- Monitor blood glucose closely if diabetic
Calcium channel blockers
Common examples:
- amlodipine
- nifedipine
- diltiazem
- verapamil
Common uses:
- Hypertension
- Angina
- Rate control for some dysrhythmias
Key side effects:
- Hypotension
- Dizziness
- Peripheral edema
- Headache
- Constipation, especially verapamil
- Bradycardia with diltiazem or verapamil
NCLEX warning
Do not lump all calcium channel blockers together.
Diltiazem and verapamil affect heart rate more than amlodipine.
Nitrates
Examples:
- nitroglycerin
- isosorbide mononitrate
Common uses:
- Angina
- Acute chest pain protocols
- Chronic angina prevention
Key side effects:
- Headache
- Hypotension
- Dizziness
- Reflex tachycardia
Critical interaction:
Do not combine nitrates with phosphodiesterase-5 inhibitors such as sildenafil, tadalafil, or vardenafil.This can cause severe hypotension.
Digoxin
Digoxin is high-yield because it links heart rate, potassium, toxicity, and therapeutic drug monitoring.
Common uses:
- Heart failure
- Atrial fibrillation rate control in some clients
Nursing checks:
- Apical pulse for one full minute
- Potassium
- Digoxin level when ordered
- Kidney function
- Toxicity symptoms
Common NCLEX hold clue:
Adult apical pulse less than 60/minToxicity signs:
- Nausea
- Vomiting
- Anorexia
- Fatigue
- Confusion
- Bradycardia
- Yellow-green visual halos
- Dysrhythmias
Potassium link:
Hypokalemia increases digoxin toxicity risk.Digoxin example
A client receives digoxin and furosemide. The potassium is 3.0 mEq/L.
Best action:
Hold digoxin and notify the provider.Rationale:
Hypokalemia increases the risk of digoxin toxicity and dysrhythmias.Diuretics
Diuretics are high-yield because they change electrolytes, fluid volume, blood pressure, and fall risk.
Loop diuretics
Examples:
- furosemide
- bumetanide
- torsemide
Key risks:
- Hypokalemia
- Hyponatremia
- Dehydration
- Hypotension
- Ototoxicity, especially with high IV doses or other ototoxic drugs
Teaching:
Take in the morning if prescribed daily. Monitor weight. Report dizziness, muscle weakness, palpitations, or hearing changes.Thiazide diuretics
Examples:
- hydrochlorothiazide
- chlorthalidone
Key risks:
- Hypokalemia
- Hyponatremia
- Hyperglycemia
- Hyperuricemia
- Photosensitivity
Potassium-sparing diuretics
Examples:
- spironolactone
- eplerenone
- triamterene
Key risks:
- Hyperkalemia
- Spironolactone can cause gynecomastia
Teaching:
Avoid potassium supplements and salt substitutes unless prescribed.Statins
Examples:
- atorvastatin
- simvastatin
- rosuvastatin
- pravastatin
Key risks:
- Muscle injury
- Elevated liver enzymes
- Rare rhabdomyolysis
Priority teaching:
Report unexplained muscle pain, tenderness, weakness, dark urine, or yellowing of the skin/eyes.Anticoagulants, antiplatelets, and hematology medications
Anticoagulants are high-alert medications.
NCLEX tests bleeding risk, lab monitoring, antidotes, and teaching.
Heparin
Routes:
- IV infusion
- Subcutaneous injection
Monitoring:
- aPTT or anti-Xa depending on protocol
- Platelets
- Signs of bleeding
Antidote:
Protamine sulfateMajor risks:
- Bleeding
- Heparin-induced thrombocytopenia
HIT red flag
A rapid drop in platelets after heparin exposure can suggest heparin-induced thrombocytopenia.
This is not just “low platelets.”
It can cause dangerous clotting.
Enoxaparin
Enoxaparin is a low-molecular-weight heparin.
Common uses:
- DVT prevention
- DVT/PE treatment
- Some acute coronary syndrome protocols
Nursing considerations:
- Usually given subcutaneously
- Do not expel air bubble from prefilled syringe unless policy says otherwise
- Do not massage site
- Monitor bleeding
- Monitor platelets
- Renal dosing matters
Warfarin
Warfarin is an oral anticoagulant.
Monitoring:
PT/INRCommon therapeutic INR:
Often 2.0 to 3.0, depending on indication.Antidote:
Vitamin KTeaching:
- Keep vitamin K intake consistent
- Do not suddenly avoid all greens
- Use soft toothbrush
- Use electric razor
- Report bleeding
- Avoid pregnancy
- Check before taking OTC medications or herbal supplements
- Many drug interactions exist
Warfarin teaching example
Incorrect teaching:
Avoid all green vegetables.Better teaching:
Keep vitamin K intake consistent and follow the prescribed INR monitoring plan.Direct oral anticoagulants
Examples:
- apixaban
- rivaroxaban
- dabigatran
- edoxaban
Key safety points:
- Bleeding risk
- Renal function matters
- Adherence matters because missed doses reduce protection
- Reversal agents vary by drug and facility access
Teaching:
Take exactly as prescribed. Do not stop without prescriber guidance. Report bleeding, black stools, severe headache, weakness, or falls.Antiplatelet medications
Examples:
- aspirin
- clopidogrel
- ticagrelor
Key risks:
- Bleeding
- Bruising
- GI irritation with aspirin
- Shortness of breath with ticagrelor in some clients
Teaching:
Report signs of bleeding. Do not stop antiplatelet therapy after a stent unless instructed by the prescriber.Endocrine medications and insulin safety
Endocrine pharmacology is high-yield because it involves blood glucose, timing, meals, and emergency symptoms.
Insulin: know onset, peak, duration
Insulin questions often test peak time because the peak is when hypoglycemia risk is highest.
| Insulin type | Examples | Onset | Peak | Duration | NCLEX safety clue |
|---|---|---|---|---|---|
| Rapid-acting | lispro, aspart, glulisine | About 15 min | 1-2 hr | 3-5 hr | Give with meals; hypoglycemia soon after |
| Short-acting | regular insulin | 30-60 min | 2-4 hr | 5-8 hr | Only insulin commonly given IV |
| Intermediate-acting | NPH | 1-2 hr | 4-12 hr | 18-24 hr | Cloudy insulin; peak can cause later hypoglycemia |
| Long-acting | glargine, detemir, degludec | 1-2 hr | Minimal/no peak | About 24 hr or longer | Do not mix with other insulin |
Hypoglycemia
Common signs:
- Sweating
- Tremor
- Hunger
- Palpitations
- Anxiety
- Confusion
- Weakness
- Seizure
- Loss of consciousness
Immediate action depends on consciousness and facility protocol.
NCLEX pattern:
Awake and able to swallow: give fast-acting carbohydrate.
Unconscious or unable to swallow: do not give oral intake; anticipate glucagon or IV dextrose per protocol/order.Metformin
Common use:
- Type 2 diabetes
Key safety concerns:
- GI upset
- Kidney function
- Lactic acidosis risk, rare but serious
- Contrast procedure policies vary
Teaching:
Take with meals to reduce GI upset. Follow instructions about holding medication around contrast studies or acute illness if directed.Sulfonylureas
Examples:
- glipizide
- glyburide
- glimepiride
Key risk:
HypoglycemiaTeaching:
Eat regular meals. Know signs of hypoglycemia. Avoid skipping meals after taking the medication.SGLT2 inhibitors: -gliflozin
Examples:
- empagliflozin
- dapagliflozin
- canagliflozin
Key risks:
- Genital infections
- Urinary tract infections
- Dehydration
- Hypotension
- Ketoacidosis warning, sometimes with only moderately elevated glucose
Teaching:
Maintain hydration. Report painful urination, genital symptoms, vomiting, abdominal pain, or rapid breathing.GLP-1 receptor agonists: -tide
Examples:
- semaglutide
- liraglutide
- dulaglutide
Key risks:
- Nausea
- Vomiting
- Delayed gastric emptying
- Pancreatitis warning signs
- Hypoglycemia risk increases when combined with insulin or sulfonylureas
Teaching:
Report severe abdominal pain that may radiate to the back, persistent vomiting, or signs of dehydration.Levothyroxine
Common use:
- Hypothyroidism
Teaching:
- Take in the morning on an empty stomach
- Take consistently
- Separate from calcium, iron, and some antacids
- Effects take time
- Report chest pain, palpitations, or signs of hyperthyroidism
Signs dose may be too high:
- Tachycardia
- Heat intolerance
- Weight loss
- Anxiety
- Insomnia
Corticosteroids
Examples:
- prednisone
- methylprednisolone
- hydrocortisone
Key risks:
- Hyperglycemia
- Infection risk
- Fluid retention
- Hypertension
- Mood changes
- GI irritation
- Osteoporosis with long-term use
- Adrenal suppression
Teaching:
Do not stop long-term corticosteroids suddenly. Report fever or infection signs. Monitor glucose if diabetic.Respiratory medications
Respiratory meds connect to airway, breathing, oxygenation, and side effects such as tachycardia.
Short-acting beta-2 agonists
Example:
- albuterol
Use:
- Rescue bronchodilator for acute bronchospasm
Side effects:
- Tachycardia
- Tremor
- Nervousness
- Palpitations
Teaching:
Use rescue inhaler for acute symptoms. If needing it more often than prescribed, seek follow-up.Long-acting beta-2 agonists
Examples:
- salmeterol
- formoterol
Safety:
Not for sudden acute symptoms.Anticholinergic inhalers
Examples:
- ipratropium
- tiotropium
Side effects:
- Dry mouth
- Urinary retention caution
- Glaucoma caution if mist gets in eyes
Inhaled corticosteroids
Examples:
- fluticasone
- budesonide
Key teaching:
Rinse mouth after use to reduce oral candidiasis risk.Theophylline
Theophylline is less common clinically than in older teaching materials, but NCLEX may still test therapeutic levels and toxicity.
Therapeutic range often taught:
10-20 mcg/mLToxicity signs:
- Nausea
- Vomiting
- Tremor
- Tachycardia
- Dysrhythmias
- Seizures
Antibiotics and anti-infectives
Antibiotic questions often test allergy, organ toxicity, superinfection, and patient teaching.
Penicillins: -cillin
Examples:
- amoxicillin
- ampicillin
- piperacillin-tazobactam
Key concerns:
- Allergy
- Anaphylaxis
- Diarrhea
- C. difficile warning with significant diarrhea
Teaching:
Report rash, wheezing, swelling, or severe diarrhea.Cephalosporins: cef- or ceph-
Examples:
- cephalexin
- ceftriaxone
- cefepime
Key concerns:
- Allergy
- Diarrhea
- C. difficile warning
- Renal dosing for some agents
Macrolides
Examples:
- azithromycin
- clarithromycin
- erythromycin
Key concerns:
- GI upset
- QT prolongation risk
- Drug interactions, especially clarithromycin and erythromycin
Tetracyclines: -cycline
Examples:
- doxycycline
- tetracycline
Key teaching:
- Photosensitivity precautions
- Take with full glass of water
- Avoid taking with calcium, iron, antacids, or dairy near the dose depending on instructions
- Avoid in pregnancy and young children unless specifically prescribed
Fluoroquinolones: -floxacin
Examples:
- ciprofloxacin
- levofloxacin
- moxifloxacin
Key risks:
- Tendon injury or rupture
- Peripheral neuropathy
- CNS effects
- QT prolongation
- Dysglycemia
- Aortic aneurysm/dissection warnings in certain at-risk patients
Teaching:
Report tendon pain, swelling, numbness, tingling, confusion, severe diarrhea, or palpitations.Aminoglycosides
Examples:
- gentamicin
- tobramycin
- amikacin
Key risks:
- Nephrotoxicity
- Ototoxicity
- Neuromuscular blockade risk in some clients
Monitoring:
- Kidney function
- Peak/trough levels when ordered
- Hearing changes
- Balance changes
- Urine output
Priority teaching:
Report ringing in ears, hearing changes, dizziness, or decreased urine output.Vancomycin
Key risks:
- Nephrotoxicity
- Ototoxicity
- Infusion reaction if infused too quickly
- Need for drug-level monitoring depending on protocol
Infusion reaction clues:
- Flushing
- Itching
- Rash
- Hypotension
Nursing action:
Stop or slow infusion according to protocol and notify the provider if reaction occurs.Sulfonamides
Example:
- trimethoprim-sulfamethoxazole
Key risks:
- Allergy
- Rash
- Stevens-Johnson syndrome
- Photosensitivity
- Hyperkalemia in some clients
- Kidney concerns
Teaching:
Report rash, sore throat, fever, mouth sores, or skin peeling.Metronidazole
Teaching:
Avoid alcohol during therapy and for the recommended period after therapy, depending on instructions.Side effects:
- Metallic taste
- GI upset
- Dark urine can occur
Psychiatric medications
Psych meds are high-yield because they test safety monitoring, toxicity, black box warnings, and therapeutic communication.
Lithium
Use:
- Bipolar disorder mood stabilization
Common therapeutic range taught for NCLEX:
0.6-1.2 mEq/LToxicity signs:
- Coarse hand tremor
- Severe diarrhea
- Vomiting
- Ataxia
- Confusion
- Slurred speech
- Seizures
Safety links:
- Dehydration increases toxicity risk
- Low sodium intake increases toxicity risk
- Kidney function matters
- NSAIDs, ACE inhibitors, and some diuretics can increase lithium levels
Teaching:
Maintain consistent fluid and sodium intake. Report vomiting, diarrhea, fever, heavy sweating, tremor, confusion, or poor coordination.SSRIs
Examples:
- sertraline
- fluoxetine
- citalopram
- escitalopram
- paroxetine
Key risks:
- GI upset
- Sexual side effects
- Insomnia or sedation
- Bleeding risk, especially with NSAIDs/anticoagulants
- Serotonin syndrome
- Suicidal thinking warning in children, adolescents, and young adults
Serotonin syndrome signs:
- Agitation
- Confusion
- Fever
- Sweating
- Tremor
- Hyperreflexia
- Diarrhea
- Muscle rigidity in severe cases
Teaching:
Do not stop abruptly. Therapeutic effect can take weeks. Report suicidal thoughts, severe agitation, fever, tremor, or confusion.MAOIs
Examples:
- phenelzine
- tranylcypromine
High-yield teaching:
Avoid tyramine-rich foods.Tyramine foods may include:
- Aged cheeses
- Cured meats
- Fermented foods
- Some wines and beers
- Some soy products
Danger:
Hypertensive crisisSymptoms:
- Severe headache
- Neck stiffness
- Palpitations
- Chest pain
- Nausea/vomiting
- Very high blood pressure
Benzodiazepines
Examples:
- lorazepam
- diazepam
- alprazolam
- clonazepam
- midazolam
Uses:
- Anxiety
- Seizure control
- Alcohol withdrawal
- Procedural sedation
- Muscle spasms depending on drug
Key risks:
- Sedation
- Respiratory depression
- Falls
- Dependence
- Withdrawal
- Increased danger with opioids, alcohol, or other CNS depressants
Antidote:
FlumazenilAntipsychotics
Examples:
- haloperidol
- risperidone
- olanzapine
- quetiapine
- clozapine
Key risks:
- Extrapyramidal symptoms
- Tardive dyskinesia
- Neuroleptic malignant syndrome
- Metabolic syndrome
- QT prolongation
- Sedation
- Orthostatic hypotension
Neuroleptic malignant syndrome
Priority signs:
- High fever
- Muscle rigidity
- Altered mental status
- Autonomic instability
- Elevated creatine kinase
This is an emergency.
Clozapine
Key risk:
AgranulocytosisTeaching:
Report fever, sore throat, or infection symptoms.Neurologic medications
Phenytoin
Use:
- Seizure prevention
Therapeutic range commonly taught:
10-20 mcg/mLKey side effects:
- Gingival hyperplasia
- Ataxia
- Nystagmus
- Sedation
- Rash
- Blood dyscrasias
- Fetal risk
Teaching:
Use good oral hygiene. Do not stop abruptly. Report rash, fever, sore throat, easy bruising, or worsening coordination.Carbamazepine
Uses:
- Seizures
- Trigeminal neuralgia
- Bipolar disorder in some cases
Key risks:
- Agranulocytosis
- Aplastic anemia
- Hyponatremia
- Rash/Stevens-Johnson syndrome
- Liver concerns
Teaching:
Report fever, sore throat, rash, mouth sores, bruising, or yellowing of skin/eyes.Valproate
Uses:
- Seizures
- Bipolar disorder
- Migraine prevention
Key risks:
- Hepatotoxicity
- Pancreatitis
- Thrombocytopenia
- Pregnancy risk
Teaching:
Report severe abdominal pain, vomiting, jaundice, unusual bleeding, or bruising.Pain medications
Pain medications are common NCLEX topics because they connect to sedation, respiratory status, liver safety, kidney safety, bleeding, and patient teaching.
Opioids
Examples:
- morphine
- hydromorphone
- oxycodone
- fentanyl
- methadone
Key risks:
- Respiratory depression
- Sedation
- Hypotension
- Constipation
- Nausea
- Urinary retention
- Dependence
- Overdose
Antidote:
NaloxoneBefore giving:
- Respiratory rate
- Sedation level
- Blood pressure
- Pain score
- Last dose and response
Priority red flag:
Respiratory rate 8/min and difficult to arouse.Action:
Hold opioid, stimulate client, support airway/breathing, notify provider or activate emergency response per protocol, and anticipate naloxone if indicated.NSAIDs
Examples:
- ibuprofen
- naproxen
- ketorolac
- celecoxib
Key risks:
- GI bleeding
- Kidney injury
- Increased blood pressure
- Fluid retention
- Cardiovascular risk
- Bleeding risk
Teaching:
Take with food if allowed. Report black stools, vomiting blood, decreased urine, swelling, chest pain, or shortness of breath.Acetaminophen
Key risk:
Liver toxicityAntidote:
N-acetylcysteineTeaching:
- Check all combination products
- Avoid exceeding daily maximum
- Avoid heavy alcohol use
- Report jaundice, right upper quadrant pain, or severe nausea/vomiting
OB and women’s health medications
Magnesium sulfate
Common use:
- Seizure prevention in preeclampsia
- Some obstetric protocols depending on indication
High-alert medication.
Monitor:
- Respiratory rate
- Deep tendon reflexes
- Urine output
- Level of consciousness
- Magnesium level when ordered
Toxicity signs:
- Loss of reflexes
- Respiratory depression
- Decreased urine output
- Hypotension
- Cardiac arrest in severe cases
Antidote:
Calcium gluconateOxytocin
Uses:
- Induction or augmentation of labor
- Postpartum hemorrhage management depending on protocol
Key risks:
- Uterine tachysystole
- Fetal distress
- Water intoxication at high doses
- Hypotension with bolus errors
Nursing focus:
- Fetal heart rate
- Contraction pattern
- Maternal vital signs
- Intake and output
Common antidotes to know for NCLEX
| Medication/toxin | Antidote or reversal agent commonly tested |
|---|---|
| Opioids | Naloxone |
| Benzodiazepines | Flumazenil |
| Heparin | Protamine sulfate |
| Warfarin | Vitamin K |
| Acetaminophen | N-acetylcysteine |
| Digoxin toxicity | Digoxin immune fab |
| Magnesium sulfate toxicity | Calcium gluconate |
| Iron overdose | Deferoxamine |
| Cholinergic crisis | Atropine |
| Anticholinesterase exposure/organophosphates | Atropine and pralidoxime depending on protocol |
Therapeutic drug levels to know
Reference ranges can vary by lab, textbook, and facility.
NCLEX questions usually use clear values when testing toxicity.
| Drug | Common NCLEX range | Toxicity clues |
|---|---|---|
| Digoxin | Often taught around 0.5-2.0 ng/mL, with lower targets often used clinically | Nausea, vomiting, anorexia, confusion, visual halos, bradycardia |
| Lithium | 0.6-1.2 mEq/L | Coarse tremor, diarrhea, vomiting, ataxia, confusion |
| Phenytoin | 10-20 mcg/mL | Nystagmus, ataxia, slurred speech, sedation |
| Theophylline | 10-20 mcg/mL in many lab references | Nausea, vomiting, tremor, tachycardia, seizures |
| Valproate | Often 50-100 mcg/mL depending on indication | Liver injury, pancreatitis, thrombocytopenia, CNS effects |
| Carbamazepine | Often 4-12 mcg/mL | Ataxia, diplopia, hyponatremia, blood dyscrasias |
| Vancomycin | Facility/protocol-specific monitoring | Kidney injury, ototoxicity, infusion reactions |
| Gentamicin | Peak/trough depend on dosing strategy | Kidney injury, ototoxicity |
Medication administration safety rules
Medication safety is one of the highest-yield parts of pharmacology.
Rights of medication administration
Common rights include:
- Right patient
- Right medication
- Right dose
- Right route
- Right time
- Right indication
- Right documentation
- Right response/evaluation
- Right education
- Right to refuse
Before giving a medication
Ask:
Is this the right patient?
Is there an allergy?
Is the dose safe?
Is the route safe?
Is the patient stable enough?
Are vital signs within parameters?
Do labs make this medication unsafe?
Is the patient able to swallow?
Is the IV site patent?
Does the medication match the diagnosis?When to question a medication order
Question or clarify when you see:
- Allergy
- Unsafe dose
- Wrong route
- Duplicate therapy
- Dangerous interaction
- Contraindication
- Missing lab value
- Abnormal vital sign
- Pregnancy risk
- Kidney or liver dysfunction
- Medication ordered for the wrong patient condition
- Unclear abbreviation
- Trailing zero or missing leading zero
- Client deterioration
Documentation rule
Do not chart medication administration before giving the medication.
Document:
- Medication given
- Dose
- Route
- Time
- Site if injection
- Client response
- Refusal if refused
- Education when relevant
- Provider notification when needed
- Adverse reaction and actions taken
For documentation examples, see NurseZee’s nursing progress notes guide and DAR charting guide.
Common NCLEX medication traps
Trap 1: Giving the medication because it is scheduled
Scheduled does not mean safe.
Example:
Metoprolol is scheduled, but the client’s heart rate is 48/min.Do not blindly give it.
Trap 2: Ignoring lab values
Example:
Spironolactone is scheduled, but potassium is 5.8 mEq/L.This raises hyperkalemia risk.
Trap 3: Confusing expected effects with emergencies
Example:
Mild dry mouth with oxybutynin is expected.
Swollen tongue after lisinopril is not expected.Trap 4: Choosing teaching when the patient is unstable
Teaching is important.
But do not choose teaching first if the patient has airway compromise, severe bleeding, hypoglycemia, or respiratory depression.
Trap 5: Missing duplicate medications
Example:
The client takes acetaminophen at home and is prescribed hydrocodone-acetaminophen in the hospital.This can create overdose risk.
How to answer NCLEX pharmacology questions
Use this sequence.
Step 1: Identify the drug class
Ask:
What class is this medication?Use suffixes and context.
Step 2: Identify why the client is taking it
Ask:
What diagnosis or symptom is this treating?This prevents random memorization.
Step 3: Check the safety data
Look at:
- Vital signs
- Labs
- Allergies
- Age
- Pregnancy status
- Kidney function
- Liver function
- Respiratory status
- Mental status
- Swallowing ability
Step 4: Decide if this is expected, unsafe, or therapeutic
Expected:
Mild headache after nitroglycerin.Unsafe:
Severe hypotension after nitroglycerin.Therapeutic:
Chest pain relieved after nitroglycerin and provider-directed treatment.Step 5: Choose the nursing action
Options may include:
- Assess
- Hold medication
- Give medication
- Notify provider
- Implement safety precautions
- Teach
- Reassess
- Document
Use the nursing process.
Assess first when data are incomplete and the client is stable.
Act first when airway, breathing, circulation, severe hypoglycemia, severe bleeding, or immediate safety is threatened.
NGN pharmacology strategy
Next Gen NCLEX pharmacology questions often provide a chart.
You may see:
- Medication administration record
- Vital signs
- Lab results
- Nurses’ notes
- Provider orders
- Allergies
- Intake and output
- ECG strip
- Patient statements
Do not read passively.
Use this structure.
Medication → expected effect → danger labs/vitals → patient cue → nursing action → evaluationExample cue cluster
Medication: Heparin infusion
Platelets: dropped from 240,000 to 85,000/mm3
Client reports new calf pain
aPTT: elevatedClinical judgment:
Recognize cues: platelet drop and new calf pain.
Analyze cues: possible heparin-induced thrombocytopenia with clotting risk.
Prioritize hypothesis: serious adverse reaction.
Take action: stop/hold heparin per protocol and notify provider immediately.
Evaluate: monitor bleeding/clotting signs, new orders, and labs.High-yield NCLEX medication categories by body system
Cardiovascular
Know:
- ACE inhibitors
- ARBs
- Beta-blockers
- Calcium channel blockers
- Nitrates
- Digoxin
- Diuretics
- Statins
- Antiarrhythmics
Priority concerns:
- Blood pressure
- Pulse
- Potassium
- Kidney function
- Dysrhythmias
- Chest pain
- Angioedema
- Digoxin toxicity
Respiratory
Know:
- Albuterol
- Ipratropium
- Tiotropium
- Inhaled corticosteroids
- Systemic corticosteroids
- Theophylline
- Leukotriene modifiers
Priority concerns:
- Airway
- Breathing
- Rescue vs maintenance inhalers
- Oral candidiasis prevention
- Theophylline toxicity
Endocrine
Know:
- Insulin types
- Metformin
- Sulfonylureas
- SGLT2 inhibitors
- GLP-1 receptor agonists
- Levothyroxine
- Methimazole/PTU
- Corticosteroids
Priority concerns:
- Hypoglycemia
- Meal timing
- Kidney function
- Thyroid over/under-treatment
- Infection risk with steroids
Hematology
Know:
- Heparin
- Enoxaparin
- Warfarin
- DOACs
- Aspirin
- Clopidogrel
- Thrombolytics
- Iron
Priority concerns:
- Bleeding
- INR
- aPTT/anti-Xa
- Platelets
- Antidotes
- Fall prevention
- Vitamin K consistency
Neuro/psych
Know:
- Lithium
- SSRIs
- MAOIs
- Benzodiazepines
- Antipsychotics
- Phenytoin
- Carbamazepine
- Valproate
- Levetiracetam
Priority concerns:
- Suicide risk
- Serotonin syndrome
- NMS
- Lithium toxicity
- Seizure control
- Blood dyscrasias
- Sedation and falls
Anti-infectives
Know:
- Penicillins
- Cephalosporins
- Macrolides
- Tetracyclines
- Fluoroquinolones
- Aminoglycosides
- Vancomycin
- Sulfonamides
- Metronidazole
- TB medications
Priority concerns:
- Allergy
- Kidney function
- Ototoxicity
- Severe diarrhea
- Tendon injury
- Liver injury
- Drug interactions
- Completing therapy
Practice questions: NCLEX pharmacology
Question 1
The nurse is preparing to administer digoxin to an adult client. Which finding is the priority reason to hold the medication and notify the provider?
- Blood pressure 138/82 mm Hg
- Apical pulse 52/min
- Respiratory rate 18/min
- Potassium 4.2 mEq/L
Answer
2. Apical pulse 52/minRationale
Digoxin can slow the heart rate. An adult apical pulse below 60/min is a common NCLEX hold parameter and requires follow-up before administration.Question 2
A client taking lisinopril reports swelling of the lips and tongue. What should the nurse do first?
- Teach the client that dry mouth is expected
- Hold the medication and assess airway
- Give the next dose with food
- Encourage fluids
Answer
2. Hold the medication and assess airwayRationale
Lip and tongue swelling may indicate angioedema, a potentially life-threatening airway emergency.Question 3
The nurse is reviewing morning medications. Which medication should the nurse question?
- Furosemide for a client with potassium 2.9 mEq/L
- Sertraline for a client with depression
- Acetaminophen for a client with temperature 38.2°C
- Docusate for a client taking opioids
Answer
1. Furosemide for a client with potassium 2.9 mEq/LRationale
Furosemide can worsen hypokalemia. Potassium 2.9 mEq/L is unsafe and increases dysrhythmia risk.Question 4
A client receiving heparin has a platelet count that dropped from 260,000/mm3 to 88,000/mm3. Which action is most appropriate?
- Administer the next heparin dose
- Hold heparin and notify the provider
- Encourage foods high in vitamin K
- Recheck the platelet count next month
Answer
2. Hold heparin and notify the providerRationale
A significant platelet drop can indicate heparin-induced thrombocytopenia, a serious complication that can increase clotting risk.Question 5
A client taking warfarin asks if they must stop eating spinach. Which response is best?
- “Yes, avoid all green vegetables.”
- “Eat a consistent amount of vitamin K-containing foods.”
- “Only eat spinach on the day you take warfarin.”
- “Vitamin K does not affect warfarin.”
Answer
2. “Eat a consistent amount of vitamin K-containing foods.”Rationale
Warfarin teaching focuses on consistent vitamin K intake, not eliminating all vitamin K foods.Question 6
A client receiving morphine is difficult to arouse. Respiratory rate is 7/min. What is the priority action?
- Document the finding
- Give the next dose in 30 minutes
- Hold the opioid and support breathing
- Encourage oral fluids
Answer
3. Hold the opioid and support breathingRationale
Respiratory depression is a life-threatening opioid adverse effect. The nurse should hold the medication, support airway/breathing, escalate per protocol, and anticipate naloxone if indicated.Question 7
A client taking lithium reports vomiting, severe diarrhea, and unsteady gait. Which action should the nurse take first?
- Tell the client to take lithium with food
- Hold the medication and notify the provider
- Encourage a low-sodium diet
- Give the next dose at bedtime
Answer
2. Hold the medication and notify the providerRationale
Vomiting, severe diarrhea, and ataxia are signs of possible lithium toxicity. Dehydration can increase lithium levels.Question 8
Which teaching is most important for a client using an inhaled corticosteroid?
- Use it only for sudden shortness of breath
- Rinse the mouth after each use
- Stop when symptoms improve
- Expect orange urine
Answer
2. Rinse the mouth after each useRationale
Inhaled corticosteroids can increase risk for oral candidiasis. Rinsing the mouth reduces this risk.Question 9
Which client should the nurse assess first?
- Client taking metronidazole with a metallic taste
- Client taking rifampin with orange urine
- Client taking fluoxetine with fever, tremor, and hyperreflexia
- Client taking iron with dark stools
Answer
3. Client taking fluoxetine with fever, tremor, and hyperreflexiaRationale
Fever, tremor, and hyperreflexia suggest serotonin syndrome, a potentially life-threatening medication reaction.Question 10
A client taking ciprofloxacin reports sudden Achilles tendon pain. What should the nurse teach?
- Continue the medication and increase exercise
- Report the symptom promptly and avoid strenuous activity
- Take the medication with calcium supplements
- This is expected and harmless
Answer
2. Report the symptom promptly and avoid strenuous activityRationale
Fluoroquinolones carry warnings for tendon injury and rupture. Tendon pain requires prompt follow-up.Pharmacology study plan for NCLEX
Week 1: Medication safety foundation
Study:
- Rights of medication administration
- High-alert medications
- Allergies and contraindications
- Medication reconciliation
- Lab and vital sign safety checks
Practice:
20 medication safety questions per day
Review every rationale
Track missed labs and hold parametersWeek 2: Cardiac and anticoagulants
Study:
- ACE inhibitors
- ARBs
- Beta-blockers
- Calcium channel blockers
- Diuretics
- Digoxin
- Nitrates
- Heparin
- Warfarin
- DOACs
Practice:
Focus on pulse, BP, potassium, INR, aPTT, platelets, bleeding, and antidotes.Week 3: Endocrine and respiratory
Study:
- Insulin timing
- Diabetes meds
- Thyroid meds
- Steroids
- Albuterol and inhalers
- Theophylline
Practice:
Drill insulin peaks and hypoglycemia interventions.Week 4: Psych, neuro, antibiotics, and pain
Study:
- Lithium
- SSRIs
- MAOIs
- Benzodiazepines
- Antipsychotics
- Anticonvulsants
- Antibiotics
- Opioids
- NSAIDs
- Acetaminophen
Practice:
Use mixed NCLEX questions and NGN case studies.Ongoing: Flashcard method
Use this format.
Generic name:
Class:
Suffix clue:
Used for:
Before giving, check:
Major side effects:
Life-threatening red flag:
Labs:
Antidote:
Patient teaching:
NCLEX trap:Quick NCLEX pharmacology cheat sheet
Hold or question the medication when you see
- Heart rate too low for beta-blocker or digoxin
- Systolic BP too low for antihypertensive
- Potassium too low for digoxin or loop diuretic
- Potassium too high for ACE inhibitor, ARB, or spironolactone
- INR too high for warfarin
- Platelets dropping on heparin
- Respiratory depression with opioids or sedatives
- Kidney dysfunction with aminoglycosides, vancomycin, lithium, metformin, or digoxin
- Liver dysfunction with acetaminophen, statins, valproate, or isoniazid
- Pregnancy with ACE inhibitors, ARBs, warfarin, isotretinoin, or some anticonvulsants
- Allergy to the medication
- New rash, skin peeling, or mucosal sores
- Signs of anaphylaxis or angioedema
Report immediately
- Trouble breathing
- Facial/tongue swelling
- Severe bleeding
- Black tarry stools with anticoagulants
- Sudden severe headache on anticoagulants
- Severe hypoglycemia
- Serotonin syndrome signs
- NMS signs
- Lithium toxicity signs
- Digoxin toxicity signs
- Tendon pain on fluoroquinolones
- Hearing loss with aminoglycosides
- Respiratory rate below safe parameters after opioid
Common antidotes
- Opioids: naloxone
- Benzodiazepines: flumazenil
- Heparin: protamine sulfate
- Warfarin: vitamin K
- Acetaminophen: N-acetylcysteine
- Digoxin: digoxin immune fab
- Magnesium sulfate: calcium gluconate
Frequently asked questions about NCLEX pharmacology
How much pharmacology is on the NCLEX?
Pharmacology is not isolated to one section. Medication safety appears across patient care, prioritization, physiological adaptation, lab interpretation, and clinical judgment. The RN test plan includes Pharmacological and Parenteral Therapies as a major client-needs subcategory.
Does the NCLEX use generic or brand medication names?
The NCLEX uses generic medication names on most items. Study generic names first and use suffixes to recognize classes.
What medications should I know for NCLEX?
Start with high-yield classes: ACE inhibitors, beta-blockers, diuretics, digoxin, anticoagulants, insulin, diabetes medications, respiratory inhalers, antibiotics, lithium, SSRIs, benzodiazepines, antipsychotics, anticonvulsants, opioids, NSAIDs, and acetaminophen.
Do I need to memorize every medication?
No. Study medication classes, suffixes, safety checks, labs, side effects, contraindications, and antidotes. You will get more value from recognizing patterns than from memorizing hundreds of isolated drug names.
What are the most important drug suffixes for NCLEX?
High-yield suffixes include -pril, -sartan, -olol, -dipine, -statin, -semide, -thiazide, -prazole, -cillin, -floxacin, -cycline, -azole, -vir, -pam, -lam, and SSRI name patterns such as -oxetine, -traline, and -pram.
What are high-alert medications?
High-alert medications are drugs that can cause significant harm if used incorrectly. NCLEX-relevant examples include insulin, anticoagulants, opioids, sedatives, concentrated electrolytes, magnesium sulfate, chemotherapy, and vasopressors.
What therapeutic drug levels should I memorize?
Common NCLEX levels include digoxin, lithium, phenytoin, theophylline, and sometimes valproate or carbamazepine. Always remember that facility ranges can vary and symptoms matter.
What insulin peak times are most important?
Know that rapid-acting insulin peaks around 1-2 hours, regular insulin around 2-4 hours, NPH around 4-12 hours, and long-acting insulin has minimal or no peak. Hypoglycemia risk is highest around peak action.
What is the biggest NCLEX pharmacology mistake?
The biggest mistake is memorizing drug facts without connecting them to patient safety. Always ask what lab, vital sign, symptom, allergy, or contraindication makes the medication unsafe.
How do I answer medication questions when I do not recognize the drug?
Look for suffixes, the diagnosis, the answer choices, and safety clues. If you still do not know the drug, use nursing process and patient safety. Choose assessment or escalation when the client shows airway, breathing, circulation, neuro, severe bleeding, or severe reaction cues.
When should the nurse hold a medication on NCLEX?
Hold or question a medication when the client has unsafe vital signs, critical labs, allergy, contraindication, toxicity signs, severe adverse reaction, or a provider order that does not match the patient’s condition.
Are side effects and adverse effects the same?
Not exactly. Side effects may be expected and manageable. Adverse effects are harmful or unsafe responses that may require holding the medication, notifying the provider, or emergency action.
How should I study pharmacology if I keep forgetting drug names?
Use class-based flashcards. For each class, write the suffix, prototype drug, key side effects, safety checks, labs, antidote, and patient teaching. Practice with questions daily instead of rereading notes passively.
Are lab values important for pharmacology questions?
Yes. Labs often determine whether a medication is safe. Potassium, INR, aPTT, platelets, creatinine/eGFR, liver enzymes, glucose, and drug levels are especially important.
Where can I practice pharmacology for NCLEX?
Use mixed NCLEX-style questions, NGN case studies, and high-yield drug-class flashcards. Start with NurseZee’s pharmacology flashcards for 50 high-yield drug classes and then test yourself with practice questions.
Final thoughts
NCLEX pharmacology becomes easier when you stop trying to memorize every medication as a separate fact.
Study classes.
Learn suffixes.
Connect each drug to one safety check.
Know the life-threatening red flags.
Then practice questions until you can move from cue to action.
That is what the exam wants: safe nursing judgment.
Not perfect recall.
Safe decisions.
Sources and references
- NCSBN: 2026 NCLEX-RN Test Plan PDF
- NCSBN: 2026 NCLEX-PN Test Plan PDF
- NCLEX: Test Plans
- NCLEX: Clinical Judgment Measurement Model
- NCLEX FAQ: Generic Medication Names
- NCSBN: Generic and Trade Names on NCLEX Items
- ISMP: High-Alert Medications in Acute Care Settings
- ISMP: List of High-Alert Medications in Acute Care Settings PDF
- FDA: Antidepressant Medication Suicidality Warning
- FDA: Fluoroquinolone Antibiotic Safety Communication
- FDA: Opioid Analgesics and Benzodiazepines Boxed Warning Safety Measures
- MedlinePlus: Digoxin Test
- NHS Specialist Pharmacy Service: Digoxin Monitoring
- NHS Specialist Pharmacy Service: Phenytoin Monitoring
- NHS Specialist Pharmacy Service: Theophylline Monitoring
- American Diabetes Association: Standards of Care in Diabetes
- Institute for Safe Medication Practices: Medication Safety Tools
- NurseZee: Pharmacology Flashcards for 50 High-Yield Drug Classes
- NurseZee: NCLEX Prep
- NurseZee: NCLEX Prioritization Questions
- NurseZee: NCLEX Lab Values Cheat Sheet
- NurseZee: Nursing Progress Notes
- NurseZee Practice Questions